Sinus Lift Surgery
Ask a Question to Our Dentist
Sinus Lift Surgery
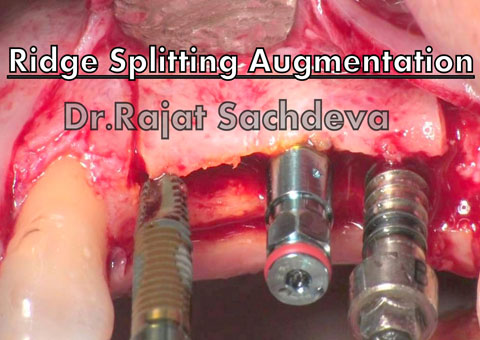
The tendency of the alveolar ridge to progressively resorb after tooth loss & typically poor quality of posterior maxillary bone, rehabilitation of this region with implant supported prosthesis has been challenging.
Anatomically maxillary sinuses are largest paranasal air cavities limited by six walls, separated from the nasal cavity, containing the neurovascular bundle & covering the tooth root by a Schneiderian membrane. The blood supply of the maxillary sinus is derived from the branches of maxillary artery, posterior superior artery, infraorbital artery & descending palatine artery. Anatomical knowledge of sinus vascularization is necessary to prevent bleeding complications during the sinus lift procedure.
Therefore, the surgical procedure of maxillary sinus lift has undergone considerable development & different variations with autogenous bone regarded as the preferred option.
Factors to satisfy the criteria for sinus augmentation are:-
-residual bone 10mm in height
-absent pathological condition/fibrous scars
-absence of multiple maxillary teeth & need for strong sinus floor for multiple implants
Preexisting local pathological conditions is an absolute contradiction to sinus lift procedure as grafting procedure can lead to fluid stagnation & exacerbated sinusitis.
At present there are two surgical approaches for maxillary sinus floor lift procedure.
First the lateral antrostomy (traumatic) being classical one described by tatum.The transcrestal approach has less morbidity but nevertheless it requires enough residual bone height for primary stability of implants i.e. prerequisite residual bone height should be 6mm to enable placement of implant 10mm in height. It is indeed a one stage procedure & less time consuming but as every procedure has its own pros & cons, its drawback is that only 2-4mm of bone height can be increased & its highly technique sensitive.
More recently, second approach i.e. crestal one (atraumatic or conservative) has been advocated by Summers using osteotomes.It includes same procedure as that of lateral approach with a crestal incision followed by full thickness flap raised & implant site prepared 1-2mm shorter than the subantral bone height using drills & osteotomes while in lateral approach antrostomy is performed using a round bur to create a U-shaped trapdoor on a lateral buttress of the maxilla.
The main advantage of this approach being less invasive procedure, improves the density of the maxillary bone allowing greater stability of implants which can be unproven if the residual bone height is 6mm.
Restoring edentulism with dental implants needs careful treatment planning especially in the posterior maxilla where the pneumatized maxillary sinuses can limit the amount of alveolar bone for implant placement. Hence maxillary sinus floor lift offers the most common & predictable preprosthetic procedures to address this problem.
Clinical Services
- Laser Dentistry
- Implantology
- Cerec One Visit Dentistry
- Componeers
- Teeth Whitening
- Cosmetic Dentistry
- Kids Dentistry
- Crown/Bridges/Dentures
- Gum Disease Treatment
- Teeth Straightening
- Invisalign Braces
- Painless Root Canals
- Wisdom tooth removal
- Full Mouth Rehabilitation
- Sterilization and Disinfection
- Stem Cell Studio
- Wedding Makeover
- Dental Clinic in Delhi

clinic
TIMINGS
Monday - Saturday
9:30 A.M.to 1:30 P.M. and
4:30 P.M. to 8:30 P.M.
Sunday
10:00 A.M. to 1:30 P.M.
Email : drrajatsachdeva@gmail.com
latest Posts
Stay up to date with all our latest news and launches.